Research Article
The Impact of Adenotonsillectomy on Health-Related Quality of Life in Paediatric Patients

Shuaib Kayode Aremu*
ENT Department, Federal Teaching Hospital, Ido-Ekiti/Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria
*Address for Correspondence: Dr. Shuaib Kayode Aremu, ENT Department, Federal Teaching Hospital, Ido-Ekiti/Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria, Tel: +2348033583842; Email: [email protected]
Dates: Submitted: 10 September 2018; Approved: 24 September 2018; Published: 25 September 2018
How to cite this article: Aremu SK. The Impact of Adenotonsillectomy on Health-Related Quality of Life in Paediatric Patients. J Adv Pediatr Child Health. 2018; 1: 006-011. DOI: 10.29328/journal.japch.1001002
Copyright License: © 2018 Aremu SK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Adenotonsillectomy; Health-related quality of life; Obstructive adenotonsillar hyperplasia

Abstract
Objective: To determine the impact of Adenotonsillectomy on Health-related quality of life (HRQoL) in children’s before and after surgery.
Study Design: Prospective, Observational, before and after the trial. 142 children who underwent Adenotonsillectomy were included in the study. Parents were made to fill pre and post-operative questionnaires which were customized from Tonsil and Adenoid health status instrument (TAHSI) and HR-QoL (Health-related quality of life) forms, one day prior to the surgery and 6 months after the surgery respectively, and the results were tabulated and analyzed.
Setting: Tertiary pediatric otolaryngology practices.
Result: Out of the 142 children in the study, 80 were male and 62 were female. Male to Female ratio is 1.3:1. Age group 1-4 years had the highest number of patients while the age group 9-12 had the least. Preoperatively the Mean score of the domain for Sleep disturbances, Physical Symptoms, Emotional distress, Daytime functions, and Caregiver concern was 14.1, 15.83, 6.89, 7.54, and 13.78 respectively. After 6 months of the surgery, the score decreased to 4.65, 4.22, 4.32, 3.1 and 4.2 respectively. This shows a significant improvement in the symptom complex and the quality of the life.
Conclusion: Adenotonsillectomy definitely leads to an improvement in the HRQoL in children as the majority of parents were extremely satisfied with the surgical outcome. Almost all of the parents reported a decrease in Sleep disturbances, Physical Symptoms, Emotional distress, Daytime functions, and Caregiver concern
Introduction
Globally, Adenotonsillectomy is arguably the most performed surgery by the pediatric otolaryngologist [1]. Its main indications are: obstructive sleep apnoea syndrome (OSAS), recurrent acute streptococcal pharyngotonsillitis, recurrent middle ear infections, hearing impairment, and, in selected cases, periodic fever with aphthous stomatitis, pharyngitis and adenopathy (PFAPA); all of these conditions have significant repercussions on the quality of life (QoL) of patients and their families [2,3]. Generally, the greatest concern of any disease to the physician, patients, and caregivers refer to its physical consequences. However, the impact of a disease on the quality of life (QoL) of a patient, or his/her parent/guardian, should also be taken into account when choosing treatment approaches.
The palatine tonsils, nasopharyngeal tonsils (adenoid), tubal and lingual tonsils are the structures which form the Waldeyer’s ring and are part of Mucosal Associated Lymphoid Tissue (MALT)/ Nasal Associated Lymphoid Tissue (NALT) system. This aggregation of lymphoid tissue is found at the entrance of the upper aerodigestive tract. As such, the tonsils and adenoids are the body’s first line of defense for the protection of the lower airways and the gastrointestinal tract, as well as for the development of antigenic memory by the host [4,5]. The principal disturbances of the tonsils and adenoid are infection and hyperplasia.
Over years controversy exists as to the effect of removing tonsils and adenoid in children as they form an important part of the immune system implicating their removal only when the benefits of alleviating the preoperative morbidity outweigh the risks of surgery and the loss of the first line of defense of the aerodigestive system [6]. But it is found that in long-term, Adenotonsillectomy only removes the nidus for stimulated cellular and humoral immunity seen in tonsillitis, without any effect on the patient’s normal immune function [7-9].
This study aims to determine the impact of Adenotonsillectomy on Health-related quality of life (HRQoL) in children’s before and after surgery using questionnaires which were customized from Tonsil and Adenoid health status instrument (TAHSI) and HR-QoL (Health-related quality of life) forms. A detailed form of Health-related quality of Life questionnaire is attached in the Appendix.
Materials and Methods
This is a prospective, observational, before and after trial study
Inclusion Criteria: A total of 142 children (80 boys and 62 girls, Male to female ratio were 1.3:1) between 1 - 12 years of age who underwent Adenotonsillectomy from May 2016 to July 2018 by the conventional dissection and snare method were included in the study. Children who underwent isolated adenoidectomy, isolated tonsillectomy were also included in the study. Demographic data (age and sex) and tonsillar size were recorded for all patients, including those whose caregivers refused enrolment or dropped out of the study.
Exclusion Criteria: Children less than 1-year-old or Children more than 12 years old; Children with nasal obstruction due to other causes like septal deviation, allergic rhinitis, nasal injury, and congenital nasal deformities and; Children of non-consenting parents or caregivers were excluded from the study.
Among indications for Adenotonsillectomy were included Adenotonsillar hypertrophy with obstructive symptoms and recurrent Adenotonsillitis. The study protocol was approved by the ethical committee of our institution.
Brodsky’s assessment scale for tonsillar hyperplasia was used to grade the tonsil based on the following scale: 0 indicates that the tonsils do not impinge on the airway; 1+ indicates less than 25% airway obstruction; 2+ indicates 26% to 50% airway obstruction; 3+ indicates 51% to 75% airway obstruction, and 4+ indicates more than 75% airway obstruction [10]. The degree of obstruction of the nasopharyngeal airway was classified as showing either ‘no obstruction’ (grade I), or ‘minimal’ (grade II), or ‘moderate’ (grade III), or ‘severe’ (grade IV) obstruction [11].
Parents were made to fill pre and post-operative questionnaires which were customized (as some of the parameters were not feasible for our study) from Tonsil and Adenoid health status instrument (TAHSI) and HR-QoL (Health-related quality of life) forms, one day prior to the surgery and 6 months after the surgery respectively. The results were tabulated and analyzed. Table 1 shows the TAHSI scoring system and table 2 shows 6 parameters [12] which we included in our study for assessing Health-related quality of life (HRQoL) respectively.
| Table 1: TAHSI Components (Tonsil and Adenoid Health Status Instrument) and Scoring system | |
| 6 subscales | Scoring Pattern |
|
0 – Not a problem 1 – very mild problem 2 – moderate problem 3 – fairly bad problem 4 – the severe problem |
|
|
|
|
|
|
|
|
|
|
| Table 2: Quality of life Parameters (Detail in Appendix) | ||
| Problem list | Problem scale | |
|
1 – None 2 – Hardly any of the time 3 – A little of the time 4 – Some of the time 5 – A good bit of the time 6 – Most of the time 7 – All the time |
|
|
||
|
||
|
||
|
||
Statistical analysis
Data were collated and presented in a descriptive format, tables, and graphs where appropriate. The data was entered in Microsoft Excel Workbook and was analyzed in “SPSS 10 for Windows (Statistical Packages for Social Sciences 22.0 version)” software. Chi-square test was performed to compare the significant association between categorical variables and the p-value < 0.05 was taken as statistically significant.
Results
Out of the 142 children in the study, 80 were male and 62 were female. Male to Female ratio is 1.3:1. Age group 1-4 years had the highest number of patients while the age group 9-12 had the least (Figure 1).
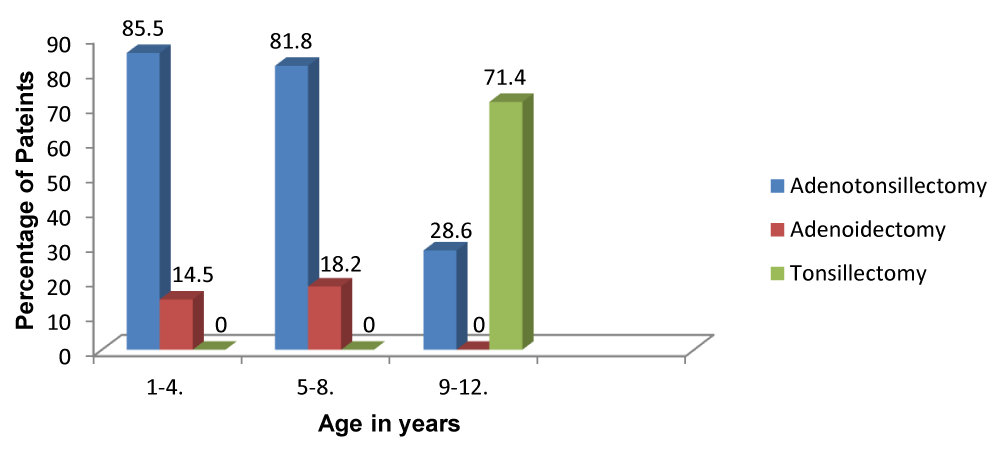
Figure 1: Distribution of type of surgery among age group.
Table 3 shows the distribution of tonsils enlargement by Brodsky grade with Grade III and Grade IV tonsils seen in 44%(63) and 13%(19) of patients respectively out of 142 total patients. Adenoidal obstruction was seen in 91% (129) of the children’s.
| Table 3: Distribution oftonsils enlargement by Brodsky grade. |
||
| Palatine tonsil | Frequency | Percentage (%) |
| 0-25%(1+) | 19 | 13.3 |
| 26-50%(2+) | 41 | 28.7 |
| 51-75%(3+) | 63 | 44.3 |
| >75%(4+) | 19 | 13.7 |
| Total | 142 | 100.0 |
Participants served as their own control as QoL changes were compared in individual participants before and after surgery. Before the surgery, the mean score of the domain was very high for all domains and the survey as a whole. After surgery, however, the mean score was low for all domains and overall survey score. This indicated that there were large improvements in QoL from before surgery to six months after surgery respectively (p = 0.0001) (Figure 2).
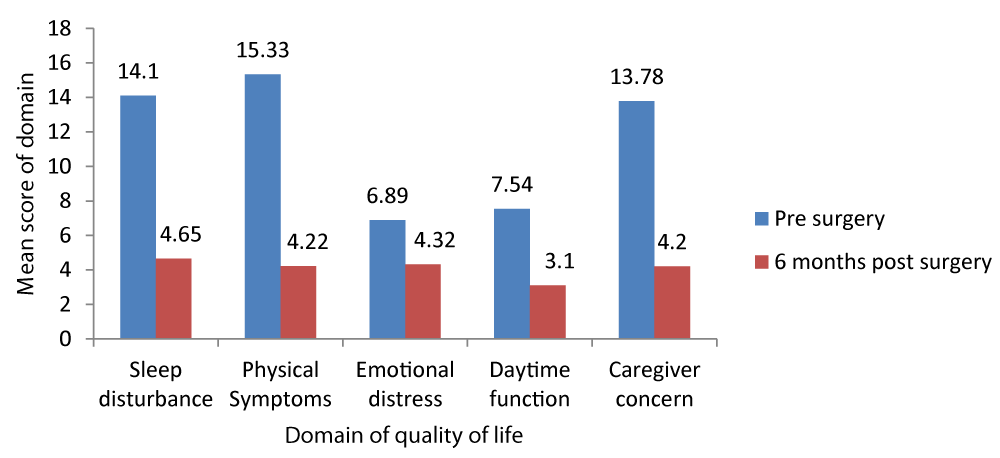
Figure 2: Comparison of mean scope of domain quality life, Pre and Post op.
Preoperatively the Mean score of the domain for Sleep disturbances, Physical Symptoms, Emotional distress, Daytime functions, and Caregiver concern was 14.1, 15.83, 6.89, 7.54, and 13.78 respectively. After 6 months of the surgery, the score decreased to 4.65, 4.22, 4.32, 3.1 and 4.2 respectively. This shows a significant improvement in the symptom complex and the quality of the life (p = 0.0001).
Primary Haemorrhage (in theatre) was encountered in 7% of cases which was effectively controlled by electrocautery and nasal packing. Reactionary (within 24 hours of surgery) Haemorrhage was seen in 2 patient who was taken back to theatre and posterior nasal packing was done as it was secondary to adenoidectomy while fortunately no cases of secondary hemorrhage (after 48hours of surgery) were encountered. There were no cases requiring re-exploration / re-admission.
Discussion
As decisions concerning resource allocation become increasingly stringent, it is important to understand the personal impact of diseases and their treatment beyond the standard medical morbidity or functional limitations so that this can be incorporated into the decision-making process. This has led to studies pertaining to outcome measures and the effect of disease and management on HRQoL.
Though Adenotonsillectomy is one of the most common surgeries performed in children [13] initially the medical line of management is started which includes analgesics for the initial 3 days followed by antibiotics like penicillin, Amox-Clav, Cephalosporins or Macrolides if symptoms persist. Surgical removal is done based on the AAP (American Academy of Paediatrics) guidelines for the indications of Adenotonsillectomy depicted in table 4. Though various surgical tools are being used apart from the cold steel like laser, cryosurgery, harmonic scalpel, radiofrequency with coblator being the latest and widely used tool, the surgical method remains the same. The postoperative morbidity and quality of life depend on multiple factors like indications of surgery, surgical technique, surgical complications and post-operative care with children generally facing lesser morbidity [14].
| Table 4: AAP indications for Adenotonsillectomy | |
| Tonsillectomy | Adenoidectomy |
|
|
This study demonstrated that adenoidectomy ± tonsillectomy was slightly more among males (56.3%) than females (43.6%) with a male to female ratio of 1.3:1. This was comparable with what that had been reported in similar studies [15-17]. However, another study demonstrated that both sexes are equally affected in the pubertal age group [18]. The mean age of children in this study was 3.9 years ± 2.64. This is smaller than what was reported by Ahmed et al, who reported age range of 0-18 years with a mean age of 5.44 years (+3.39 SD) and a median age of 5 years [19]. This finding could be because they included older children in their study.
In an Open, randomised controlled trial where 300 children between 2-8 years of age with symptoms of adenotonsillar hypertrophy /infection were divided into two groups ,one with Adenotonsillectomy and the other with watchful waiting it was found that Adenotonsillectomy could be considered an indication for surgery for children with three to six episodes of throat infection in a year and not in children with mild symptoms of adenotonsillar hypertrophy or infection as the surgical benefit did not outweigh the effects of watchful waiting in mild cases [20].
In a hospital-based prospective study by Afolabi et al. [6], the most common indication for Adenotonsillectomy was obstructive symptoms and the reduction in pre-operative symptoms recorded were from 93.1% pre-op to 10.3% post-op for recurrent sore throat, from 100 to 13.8% for sleep-disordered breathing and from 79.3% to 13.8% for eating & swallowing disturbances which is similar to our results of reduction from Mean average score of 15.83 to 4.22 for physical symptom, from 14.1 to 4.65 for sleep disturbances and from 7.54 to 3.1 for Daytime function disturbances. This study stressed the importance of parental satisfaction and that parents often expected improvement in the quality of life of the child as a whole rather than just reduction in a particular symptom which formed the indication for the surgery.
In a prospective study by Carneiro et al. [21], it was observed that parental satisfaction was significant for snoring, recurrent tonsillitis and use of antibiotics post Adenotonsillectomy similar to our study. However, rhinitis did not show significant improvement postoperatively.
Conclusion
Adenotonsillectomy definitely leads to an improvement in the HRQoL in children as the majority of parents were extremely satisfied with the surgical outcome. Almost all the parents reporteds the decrease in Sleep disturbances, Physical Symptoms, Emotional distress, Daytime functions, and Caregiver concern.
References
- Derkey CS. Pediatric otolaryngology procedures in the United States: 1977-1987. Int J Paediatr Otorhinolaryngol 25.1993; 1-12. Ref.: https://goo.gl/pRQLtG
- Darrow DH, Siemens C. Indications for tonsillectomy and adenoidectomy. Laryngoscope. 2002; 112(8 Pt 2 Suppl 100): 6–10. Ref.: https://goo.gl/8WTndo
- Bellucci LM, Marchisio P, Materia E, Passàli FM. Clinical guideline on adenotonsillectomy: the Italian experience. Adv Otorhinolaryngol. 2011; 72: 142–145. Ref.: https://goo.gl/gq3nJY
- Caulfield., Helen M. Obstructive sleep apnoea in childhood. In: Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, vol. 1. 7th ed, Michael G, George GB, Martin JB editors. Great Britain: Hodder Arnold.2008; 85: 1102-1109. Ref.: https://goo.gl/4g931W
- Peyton S, Audie LW, Brian JW. Pharyngitis and adenotonsillar disease. In: Cummings Otolaryngology, Head and Neck Surgery, 5th ed, vol.1, Paul WF, Bruce HH, Valerie JL editors. Philadelphia: Mosby Elsevier 2010; 195-197. Ref.: https://goo.gl/fV2hnZ
- Afolabi OA1, Alabi BS, Ologe FE, Dunmade AD, Segun-Busari S. Parental satisfaction with post-adenotonsillectomy in the developing world. Int J Pediatr Otorhinolaryngol. 2009; 73: 1516–1519. Ref.: https://goo.gl/wz1d2H
- Kaygusuz I, Gödekmerdan A, Karlidag T, Yalçin S, Aral I, et al. Early-stage impacts of tonsillectomy on immune functions of children. Int J Pediatr Otorhinolaryngol. 2003; 67: 1311-1315. Ref.: https://goo.gl/6tzHTZ
- Zielnik-Jurkiewicz B, Jurkiewicz D. Implication of immunological abnormalities after adenotonsillectomy. Int J Pediatr Otorhinolaryngol. 2002; 64: 127-132. Ref.: https://goo.gl/uGmDM9
- Kaygusuz I, Alpay HC, Gödekmerdan A, Karlidag T, Keles E, et al. Evaluation of long-term impacts of tonsillectomy on immune functions of children: A follow-up study. Int J Pediatr Otorhinolaryngol. 2009; 73: 445-449. Ref.: https://goo.gl/DGfpsN
- Brodsky L, Moore L, Stanievich JF. A comparison of tonsillar size and oropharyngeal dimensions in children with obstructive adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol. 1987; 13: 149-157. Ref.: https://goo.gl/Kgfgsy
- Orji FT, Okolugbo NE, Ezeanolue BC. The role of adenoidal obstruction in the pathogenesis of otitis media with effusion in Nigerian children. Niger J Med. 2010; 19: 62-68. Ref.: https://goo.gl/Befrjk
- Rosenfeld RM, Bhaya MH, Bower CM, Brookhouser PE, Casselbrant ML, et al. Impact of tympanostomy tubes on child quality of life. Arch Otolaryngol Head Neck Surg. 2000; 126: 585-592. Ref.: https://goo.gl/SeqTNG
- Derkay, Craig S. Paediatric otolaryngology procedures in the United States: 1977–1987. Int. J. Pediatr. Otorhinolaryngol. 1993; l 25: 1–12. Ref.: https://goo.gl/vm1FH8
- Piltcher OB, Scarton FB. Antibiotic use in tonsillectomies: therapeutic or prophylactic? Required or excessive? Rev Bras Otorrinolaringol. 2005; 71: 686-690. Ref.: https://goo.gl/n1Srxr
- De Serres LM1, Derkay C, Sie K, Biavati M, Jones J, et al. Impact of adenotonsillectomy on quality of life on children with obstructive sleep disorders. Arch Otolaryngol Head Neck Surg. 2002; 128: 489-496. Ref.: https://goo.gl/e26uEc
- Mitchell R, Kelly J. Quality of Life after Adenotonsillectomy for SDB in Children. Otolaryngol Head Neck Surg. 2005; 133: 569-572. Ref.: https://goo.gl/j1yFg3
- Mitchell R, Kelly J, Call E. Quality of life after adenotonsillectomy for obstructive sleep apnoea in children. Arch Otolaryngol Head Neck Surg. 2004; 130: 190–194. Ref.: https://goo.gl/vxhDws
- Lim J, Mckean MC. Adenotonsillectomy for obstructive sleep apnoea in children. Cochrane database of systemic reviews. 2011; 2: CD003136. Ref.: https://goo.gl/KiCfS8
- Ahmed AO, Aliyu I, Kolo ES. Indications for tonsillectomy and adenoidectomy: Our experience. Niger J Clin Pract. 2014; 17: 90-94. Ref.: https://goo.gl/a5cwSQ
- van Staaji BK, van den Akker EH, Rovers MM, Hordijk GJ, Hoes AW, et al. Effectiveness of adenotonsillectomy in children with mild symptoms of throat infections or adenotonsillar hypertrophy: open, randomized controlled trial. BMJ. 2004; 329:651. Ref.: https://goo.gl/zeddPd
- Carneiro LEP, Neto GCR, Camera MG. Adenotonsillectomy Effect on the Life Quality of Children with Adenotonsillar Hyperplasia. Int Arch Otorhinolaryngol. 2009; 13: 270-276. Ref.: https://goo.gl/FoSP1H