
More Information
Submitted: August 16, 2021 | Approved: September 09, 2021 | Published: September 10, 2021
How to cite this article: Tanwattanakul J, Sriprachote S, Tangpukdee J, Chanthapreeda N, Santiboon TT. Effects of food programme for enhancing obesity children healthy of their abilities and expectations to self-efficacy for preventing early childhood. J Adv Pediatr Child Health. 2021; 4: 093-100.
DOI: 10.29328/journal.japch.1001040
ORCiD: orcid.org/0000-0001-7344-206X
Copyright License: © 2021 Tanwattanakul J, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Obese children health; The affecting programs; Body mass index enhancement; Abilities and expectations; Self-efficacy; Preventing early childhood education

Effects of food programme for enhancing obesity children healthy of their abilities and expectations to self-efficacy for preventing early childhood
Jirawon Tanwattanakul1*, Suthiporn Sriprachote2, Juraporn Tangpukdee1, Nilawan Chantapreeda1 and Toansakul Tony Santiboon3
1Department of the Child Health Nursing, Faculty Nursing, Khon Kaen University, Khon Kaen, Thailand
2Professional Nurse, Children’s Ward, Kamalasai Hospital, Kamalasai, Kamalasai District, Kalasin, Thailand
3Department of SMEC, Curtin University of Technology, Perth, WA, Australia
*Address for Correspondence: Dr. Jirawon Tanwatthanakul, Associate Professor, Department of the Child Health Nursing, Faculty Nursing, Khon Kaen University, 123 Mittrapab Highway, Muang District, Khon Kaen, Thailand 40002, Email: [email protected]; [email protected]
This study aims to assess parents’ perceptions of their responses to the perceived awareness programme competency abilities and expectations for enhancing parents on weight control of their pre-school children in preventing with Obesity. It has defined self-efficacy as one’s belief in one’s ability to succeed in specific situations and accomplish a task with the theoretical framework of Bandura’s Model by quasi-experimental research in 16 weeks. To promote the self-efficacy and expectations, the 10-item Questionnaire on Self-Efficacy Program, the 22-item Questionnaire on Parents’ Efficacy Interaction, and the 46-item Questionnaire on Parental Expectations assessed parents’ perceptions. A sample size consisted of 14-pre-school children whose age ranged 2-5 years old at the Child Development Demonstration Centre, Khon Kaen University was selected. Providing knowledge, teaching, demonstration, experimentation, and organized activities were organized. Parents’ perceptions of their abilities for controlling children’s weight and height with pre- and post-experimental programmes differentiated, significantly. Parents’ responses to the post performances are over than pre-experiment for the QSEP, the QPEA, and the QPE, differently. They answered and followed up on child management with parents online for 16 weeks, continuously. The obese early childhood at the CDC Demonstration Centre, Faculty of Nursing used the food programme to self-efficacy with their parents taking part and cooperating well in specifying research objectives. There are 2,958,441 children in rural areas are lacking attention, because of food and health problems in the 19,171-Child Development Centres none yet have food programmes to prevent health and hygiene problems. Although Thailand took the next leap forward for its investment in Early Childhood Development through legislation, improved quality services, and social transfer grants for families with young children since 2018.
Overweight and obesity is defined as abnormal or excessive fat accumulation that presents a risk to health. A crude population measure of obesity is the body mass index (BMI), a person’s weight (in kilograms) divided by the square of his or her height (in meters). A person with a BMI of 30 or more is generally considered obese. A person with a BMI equal to or more than 25 is considered overweight. Once considered a problem only in high-income countries, overweight and obesity are now dramatically on the rise in low- and middle-income countries, particularly in urban settings [1]. Obesity is a leading preventable cause of death worldwide, with increasing rates in adults and children [2]. In 2015, 600 million adults (12%), and 100 million children were obese in 195 countries [3].
Obesity is mostly preventable through a combination of social changes and personal choices. Changes to diet and exercising are the main treatments. Obesity is more common in women than in men [4]. Authorities view it as one of the most serious public health problems of the 21st century [5]. Obesity is stigmatized in much of the modern world, though it was seen as a symbol of wealth and fertility at other times in history and still is in some parts of the world. A few cases are caused primarily by genes, endocrine disorders, medications, or mental disorders [6]. On average, obese people have greater energy expenditure than their normal counterparts due to the energy required to maintain an increased body mass [7].
The recommendations can inform the decisions of state and local child care regulators, child care providers, health care providers, directors of federal and local child care and nutrition programs [8]. In 2019, an estimated 38.2 million children under the age of 5 years were overweight or obese. Once considered a high-income country problem, overweight and obesity are now on the rise in low- and middle-income countries, particularly in urban settings (World Health Organization [9]. Children who have obesity are more likely to have: High blood pressure and high cholesterol, which are risk factors for cardiovascular disease, increased risk of impaired glucose tolerance, insulin resistance, and type 2 diabetes, and breathing problems [10].
Obesity in Thailand has been flagged as a major source of health concern, with 32% of the population identifying as overweight and 9% obese. Consistent with cognitive epidemiological data, numerous studies confirm that obesity is associated with cognitive deficits. Whether obesity causes cognitive deficits or vice versa is unclear at present. Therefore, obese children revealed a lot of diseases to suggest that the school organized a behavior change camp according to 3 principles, aiming to reduce obese children to 15 percent by the year 2025 [11]. Overweight and obesity are considered a serious health problem in Thailand. To examine the prevalence of overweight and obesity in a nationally representative sample of Thai children and adults in schools based on international standards and affect learning including problems with the bones causing pain in the knees, ankles, bones, legs bent, buckling legs, unable to walk easily due to too much weight as well [12].
Affecting programs for enhancing abilities and expectations to control the weight of obese children, the restricting highly desired foods can result in children responding to external cues of availability rather than internal cues of hunger and satiety. Removing all undesired foods from the house (and setting up a healthier home environment) would be a better option. Interestingly, this parenting style has also been associated with a lower prevalence of obese children. Encouraging the use of this parenting style in conjunction with specific health-promoting behaviors may have the greatest impact on the development of healthy eating and activity behaviors among children [13].
Self-efficacy is a central tenet of Albert Bandura’s (1977) social cognitive theory [14]. A central idea posed in social cognitive theory is that success experiences raise self-efficacy but repeated failures lower self-efficacy [15]. The theory of self-efficacy, as presented by Bandura [16] was outlined as a theoretical framework. The theory was based on the principle assumption that “psychological procedures, whatever their form, serve as a means of creating and strengthening expectations of personal efficacy”. The outcome and efficacy expectations are differentiated because individuals can believe that a particular course of action will produce certain outcomes [17]. Because self-efficacy typically comes into play when there is an actual or perceived threat to one’s personal safety, or one’s ability to deal with potentially aversive events. Increasing a person’s self-efficacy increases their ability to deal with a potentially adverse situation. Perceived self-efficacy mediates anxiety arousal [18].
Focused on parents who are involved in their child’s growth and development, and adopt implement model healthier behaviors themselves are more likely to be successful at preventing their child from becoming overweight or in helping they lose weight. Using the questionnaires and affecting program to assess parents with obesities’ perceptions for enhancing abilities and expectations to control the weight in preventing pre-school children with obesity that obtained with the theoretical framework of Albert Bandura’s Model [19]. Encouraging parents to increase awareness of their parents’ abilities will have to change behaviors, determinate for trying to achieve the success that they are able to result in high expectations for goals when this happens, parents are likely to succeed [20].
The single round quasi-experimental research investigated the effects of a program for promoting and enhancing parents with obesities’ perceptions and expectations program for enhancing abilities and expectations to self-efficacy in preventing pre-school children with obesity whose age ranged from 2 to 5 years old at the Child Development Demonstration Center, the Faculty of Nursing, Khon Kaen University.
Research objectives
To assess parents’ perceptions of their responses to the perceived awareness programme competency abilities and expectations for enhancing parents on weight control of their pre-school children in preventing with Obesity, which has defined self-efficacy as one’s belief in one’s ability to succeed in specific situations and accomplish a task with the theoretical framework of Bandura’s Model by quasi-experimental research in 16 weeks.
Research framework
The theoretical framework of Albert Bandura’s Model [19] defined self-efficacy as parent’s beliefs about their capabilities to produce designated levels of performance that exercise influence over events that affect their lives. A strong sense of efficacy enhances human accomplishment and personal well-being in many ways. Such an efficacious outlook fosters intrinsic interest and deep engrossment in activities. They set themselves challenging goals and maintain strong commitment to them. They heighten and sustain their efforts in the face of failure. They quickly recover their sense of efficacy after failures or setbacks. They attribute failure to insufficient effort or deficient knowledge and skills which are acquirable. They approach threatening situations with assurance that they can exercise control over them. Such an efficacious outlook produces personal accomplishments, reduces stress and lowers vulnerability to depression.
Research procedures
This research study has described four main sources of influence by which a person’s self-efficacy is developed and maintained: (a) performance accomplishments or mastery experiences; (b) vicarious experiences; (c) verbal or social persuasion; and (d) physiological, or somatic and emotional, states.
The most important factor that determines the strength of influence of an observed success or failure on one’s own self-efficacy is the degree of similarity between the observer and the model. People with high confidence in their capabilities approach difficult tasks as challenges to be mastered rather than as threats to be avoided. They set themselves challenging goals to which they are strongly committed. They heighten and sustain their efforts in the face of failure.
Data collection
After receiving research ethics in humans which have been submitted to protect the rights of children. There would be no recording of clear pictures of children that may affect children. Both the physical, mental and visual characteristics of children were cleared.
Carried out the experiment as follows:
1. Before the experiment, the parents would answer the questionnaire and weighing pre-school children who are obese.
2. Proceed with the experimental activities as follows:
The 1st week: To encourage parents to be frightened of the negative effects on children who are obese along with giving a guide to parents.
The 2nd week: To encourage parents are to have knowledge and experience in caring for children, using activities to present the amount of suitable for children who are obese. Through real media and hypothetical media, demonstration of quality evaluation of beverages, desserts, and milk for parents to try and prepare them.
The 3rd week: To create a model for parents and children who are obese with the activities of presenting models in video media, and activities to present the benefits of model media through storytelling along with giving storytelling media for parents to apply with children at home.
3. After the experiment in the 4th week, parents were asked to answer the questionnaire, and follow up on children weight management with parents every week online and in the 16th week, weigh children who are obese.
Research instruments
1. The Questionnaire on Self-Efficacy Program (QSEP)
The 10-item Questionnaire on Self-Efficacy Program (QSEP) was assessed children’s parents to promote the self-efficacy and expectations for enhancing weight control of their obese children that comprises a handbook of “Caring for 2-5-year-old pre-school children with obesity”.
The video on “Parents who successfully control the weight of obese children” was watched.
The story “Baby Bear is Afraid of Fat”, with the process of leading parents by providing knowledge, teaching, demonstration, experimentation, and organized activities for 1-2 children and their parents, with a trial period of 16 weeks and parents’ responses on five options.
2. Weight Scale Measurement (WSM)
The Weight Scale Measurement (WSM) is used to collect data weight scale standardized pass the calibration in 16 weeks were measured the children, continually.
3. Altimeter
Using the Altimeter for measuring the pre-primary children of their physical high in the pre-experiment on the first week and post-experiment on the 16th week was compared.
4. The Questionnaire on Parents’ Efficacy Interaction (QPEI).
To assess parents with obesities’ perceptions with the 22-item Questionnaire on Parents’ Efficacy Interaction (QPEI) of their affecting programs to their knowledge about obesity toward obese children for enhancing abilities to control the weight obese children in three scales, namely; Obesity Understanding (OU), Assessing Nutrition (AN), and Parental Practices (PP) scales. There are two options of parents’ answering questions and assigning scores for statistical analysis: 0 and 1 are responses to be given. If parents’ answering is right, meanwhile, the scoring is 1. If they answered wrong, it means they got a score as 0, The QPEI assessed parents in pre-experiment before they attended and post-experiment after they were going on attend of this program in 16 weeks, respectively.
5. The Questionnaire on Parental Expectations (QPE)
Adapted version from the Social Cognitive Theory (SCT) on self-regulation and self-efficacy are keyed to integrating healthier nutrition into pre-primary students’ lifestyles. The 46-item Questionnaire on Parental Expectations (QPE) was used and assessed the controlling the weight of obese children on five options Likert’s scale [21]. According to Bandura [19], there are five main sources of Self-Efficacy Beliefs; Mastery Experiences; Vicarious Experiences; Verbal Persuasion; Emotional and Physiological States scales.
Data analysis
Data analysis was analyzed with the mean score ( ), standard deviation (σ), variance (σ2), internal consistency (Cronbach Alpha Reliability) coefficient (α–reliability), F-test, t-test, simple correlation of Pearson Product Movement (r), and pre-test and post-test design.
The results are given in Table 1 which shows that on an average item mean for each of the Pre- and Post Self-Efficacy Program for the QSEP scales. For the remaining 10 items on Self-Efficacy Program scale as nature, the scale was assessed with Cronbach α-reliability coefficient.
Table 1, the QSEP is valid and reliable with Cronbach α-reliability that ranged from 0.60 to 0.63. Using the t-test, analysis was differentiated at the level of .05, significantly [22].
| Table 1: Comparisons between obese children with their parents’ perceptions of their Pre- and Post Self-Efficacy Program for the QSEP | ||||||||
| Form | S.D. | σ2 | α-reliability | F-test | Sig. | t-test | Sig. | |
| Pre Self-Efficacy | 1.61 | 0.22 | 7.25 | 0.63 | 10.80*** | .000 | 2.25 | 0.043* |
| Post Self-Efficacy | 1.82 | 0.27 | 4.60 | 0.61 | 16.08*** | .000 | ||
| N = 14, *p < .05, **p < .01, ***p < .001 | ||||||||
Using the 22-item Questionnaire on Parents’ Efficacy Ability(QPEA), parents’ perceptions with pre-experiment and post-experiment to their self-efficacy interaction was assessed in three scales, namely; Obesity Understanding, Assessing Nutrition, and Parental Practices scales (Table 2).
Table 2 showed off the parents’ responses for the QEPA scales of parents’ abilities to their self-efficacy interaction for taking care with their child obesity. It also provides to support the parent contributions’ abilities that they needed to take differences into consideration when planning and designing their affecting program, differently (ρ < 0.01).
| Table 2: Comparisons between the pre-and-post-experiment of parents’ abilities to their self-efficacy interaction for the QPEA. | ||||||||
| Scale | S.D. | σ2 | α-reliability | F-test | Sig. | t-test | Sig. | |
| Post Self-Ability | 19.14 | 2.59 | 6.75 | 0.66 | 32.51*** | .000 | 3.98 | 0.002** |
| Pre Self-Ability | 9.00 | 1.36 | 1.85 | 0.65 | 5.64*** | .000 | ||
| N = 14, *p < .05, **p < .01, ***p < .001 | ||||||||
Using the 46-item Questionnaire on Parental Expectations (QPE), parents’ perceptions of their controlling expectations toobese children was assessed on five options in five major sources;Self-Efficacy Beliefs (SEB): Mastery Experiences (MEx); Vicarious Experiences (VEx); Verbal Persuasion (VPe); and Emotional and Physiological States (EPS) scales.
In Table 3, we compared how pre-and-post-experiment of informants used inter-sentential referencing outlines. Four of five scales are positive with parents’ responses are differentiated with the t-test (ρ < 005) for the QPE scales, significantly. The EPS scale is negative. Using ANOVAanalysis (eta2) was re-analyzed the Verbal Persuasion scale which is significant, differently (ρ < 005).
| Table 3: Comparisons between pre-and-post self-efficacy programs to parents’ controlling expectations of obese child for the QPE. | ||||||||
| Scale | Form | Score mean | S.D. | α-Reliability | Simple Correl.(r) | t-test | ANOVA Result (eta2) | |
| Self-Efficacy Beliefs | Pre-Ex | 34.71 | 3.86 | 0.49 | 0.66 | 0.25 | 1.96* | 0.55 |
| Post-Ex | 37.93 | 4.21 | 0.61 | 0.88 | ||||
| Mastery Experiences | Pre-Ex | 31.86 | 3.54 | 0.61 | 0.60 | 0.14 | 2.07* | 0.91 |
| Post-Ex | 36.14 | 4.02 | 0.70 | 0.77 | ||||
| Vicarious Experiences | Pre-Ex | 31.71 | 3.52 | 0.65 | 0.78 | 0.57* | 2.46** | 0.94 |
| Post-Ex | 34.93 | 3.88 | 0.46 | 0.60 | ||||
| Verbal Persuasion | Pre-Ex | 37.29 | 4.14 | 0.55 | 0.88 | 0.85** | 0.49 | 0.98** |
| Post-Ex | 37.64 | 4.18 | 0.53 | 0.85 | ||||
| Emotional and Physiological States | Pre-Ex | 46.23 | 4.64 | 0.33 | 0.79 | 0.10 | -0.64 | 0.79 |
| Post-Ex | 45.37 | 4.54 | 0.56 | 0.91 | ||||
| Totalized analysis | Pre-Ex | 182.16 | 3.96 | 0.31 | 0.90 | 0.34* | 1.95* | 1.00** |
| Post-Ex | 191.82 | 4.17 | 0.40 | 0.94 | 0.94*** | |||
| N = 14, *p < .05, **p < .01, ***p < .001 | ||||||||
This program can cause the weight of the children after the experiment to differ from the target weight. The pre-and-post-test weight differs from the target weight ( = 19.84 and 18.62 kg, respectively). After the mean weight loss experiment reduced to 18.62, which differ at the level of .05, meanwhile this program could control child weight, significantly (Table 4).
| Table 4: Mean Average Scores, Standard Deviation, t-test for the WSM. | |||||||
| Week | Weight (Kg) | Week | Weight (Kg) | Week | Weight (Kg) | Week | Weight (Kg) |
| Pre-week | 19.97 | 5th week | 20.50 | 9th Week | 20.55 | 13th Week | 19.83 |
| 2nd Week | 20.66 | 6th week | 20.13 | 10th Week | 20.65 | 14th Week | 18.60 |
| 3rd Week | 20.29 | 7th Week | 20.59 | 11th Week | 20.25 | 15th Week | 19.83 |
| 4th Week | 20.49 | 8th Week | 20.17 | 12th Week | 20.09 | 16th Week | 18.60 |
| Total weight = 20.08 kg, S.D. = 44.48, Variance = 1978.96, α-Reliability = 0.99, F-test = 6.345***, sig.<.001, Standardized weight = 13.93 kg | |||||||
The standardized Thai’s children weight, whose age is 2-5-year-olds ( = 11.65-16.24 kg.), total mean weight is13.93 kg and standardised high ( = 88.30-108.70 cm.), total mean high as 98.98 cm. for a child boy. In terms of a child girl ( = 10.86-15.84 kg.), total mean weight is 13.27 kg, standardized high ( = 88.30-108.70 cm.), and the mean high as 97.23 cm.
Using the Weight Scale Measurement (WSM) measured the 14-pre-primary children with average means weight scale ( ), it has found that the average means weight scale as 19.98 kg, and 20.66 kg ( = 19.98 and 20.66 kg.) for pre-test and post-test measurement. Generally, the standardized weight as 13.19 kg, Tables 5 showed off the pre-primary children of their standardized weight and height in 16 weeks, continually.
As reported in Table 5, comparisons between the pre-test ( = 19.98 kg.) and the post-test of the weight ( = 20.66 kg), and most of the pre- and post weight average indicated with the standardized weight were compared. These results between pre-post experimental weights showed off differentiated, significantly (ρ < 005). The results of pre-and-post-weights are over than standardised values to collect data standardized weight passed the calibration. On the whole, these results are acceptable and confirmation which was satisfactory for further use in this study.
| Table 5: Comparisons between mean standardized weight pre-and-post-experiment designs for the WSM. | ||||||
| Trial | S.D. | Correlation | t-test | df | Sig. | |
| Post-weight | 20.66 | 2.38 | 0.91*** | 2.13* | 13 | .05 |
| Pre-weight | 19.98 | 2.87 | ||||
| Post-weight | 20.66 | 2.38 | 0.41 | 9.04*** | 13 | .000 |
| Standardized-weight | 13.19 | 1.83 | ||||
| Pre-weight | 19.98 | 2.87 | 0.34 | 11.98*** | 13 | .000 |
| Standardized-weight | 13.19 | 1.83 | ||||
| N = 14, *p < .05, **p < .01, ***p < .001 | ||||||
Figure 1 showed the profile linear graphic of the 14-pre-primary weight in 16 weeks with the Weight Standard Measurement. The graphical depiction of the line linear equation as y = - 0.084x + 20.79 (y-exist is weight values, and x-exist is time schedules in 16 week). The slope decreased, it means the affecting programs for enhancing abilities and expectations for self-efficacy in pre-and-post experimental weight as well for decreasing child›s weight obesity disease that confirmation and agreeable by the conceptual framework of Banura [19].
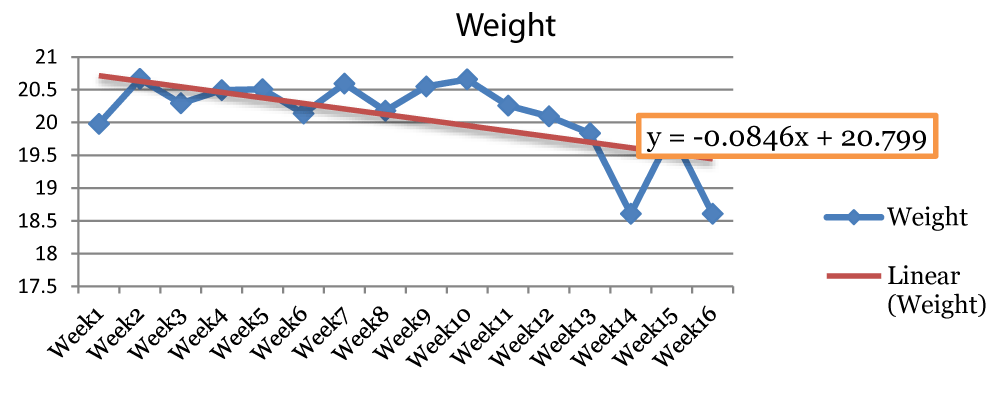
Figure 1: Correlations between children’ weights are decreasing obesity on their times, significantly.
Comparisons between mean standardized height of the 14-pre-primary children using the Altimeter for measuring the height of children in terms of before and after experimental weight program was measured.
Table 6 reported the comparisons between the 14-pre-primary children’s height of their after-before-experimental measurement with the standardized height of child Thai’s high (93.09 cm.). Using the t-test analysis was analyzed. It has found that the pair-means (before-and after measuring height, before and standard measuring height, and after and standard measuring height are the pairing mean trial), each trial is differentiated at the evidence of .05 levels of three order pairs, significantly.
| Table 6: Comparisons between mean averages standardized high in terms of before and after using program for the Altimeter (cm.). | ||||||
| Trial | S.D. | Correlation | t-test | df. | Sig. | |
| After-high | 99.68 | 7.11 | 0.99*** | 2.14* | 13 | .050 |
| Before-high | 98.25 | 6.82 | ||||
| After-high | 99.68 | 7.11 | 0.54* | 9.00*** | 13 | .000 |
| Standardized-high | 93.06 | 24.48 | ||||
| Before-high | 99.68 | 6.82 | 0.57* | 11.87*** | 13 | .000 |
| Standardized-high | 93.06 | 24.48 | ||||
| N = 14, *p < .05, **p < .01, ***p < .001 | ||||||
Research on the single round quasi-experimental was to investigate the effects of a program for promoting and enhancing parents of their perceptions to their obese children using the food expectation program to self-efficacy in preventing 14-pre-school children whose age ranged from 2 to 5 years old at the Child Development Demonstration Center, the Faculty of Nursing, Khon Kaen University, Thailand.
For children and adolescents aged 2-19 years in 2017-2018: The prevalence of obesity was 19.3% and affected about 14.4 million children and adolescents. Obesity prevalence was 13.4% among 2- to 5-year-olds, 20.3% among 6- to 11-year-olds, and 21.2% among 12- to 19-year-olds [23]. Body mass index (BMI) is a measure used to determine childhood overweight and obesity. Overweight is defined as a BMI at or above the 85th percentile and below the 95th percentile for children and teens of the same age and sex. Obesity is defined as a BMI at or above the 95th percentile for children and teens of the same age and sex. The CDC Growth Charts are the most commonly used indicator to measure the size and growth patterns of children and teens. BMI-for-age weight status categories and the corresponding percentiles were based on expert committee recommendations [24].
Childhood obesity is one of the most serious public health challenges of the 21st century. The problem is global and is steadily affecting many low- and middle-income countries,particularly in urban settings. The prevalence has increased at an alarming rate. Globally in 2016, the number of overweight children under the age of five is estimated to have been over 41 million. The prevalence of overweight and obesity in adolescents is defined according to the WHO growth reference for school-aged children and adolescents (overweight = 1 standard deviation body mass index for age and sex, and obese = 2 standard deviations body mass index for age and sex) [25].
Childhood obesity can also lead to poor self-esteem and depression. One of the best strategies to reduce childhood obesity is to improve the eating and exercise habits of your entire family. Treating and preventing childhood obesity helps protect your child’s health now and in the future. If you’re worried that your child is putting on too much weight, talk to his or her doctor. The doctor will consider your child’s history of growth and development, your family’s weight-for-height history, and where your child lands on the growth charts. This can help determine if your child’s weight is in an unhealthy range [26].
The most important strategies for preventing obesity are healthy eating behaviors, regular physical activity, and reduced sedentary activity. The Dietary Guidelines provide general diet and lifestyle recommendations for healthy children ages 2 years and over. Parents and caregivers can help prevent childhood obesity by providing healthy meals and snacks, daily physical activity, and nutrition education. Healthy meals and snacks provide nutrition for growing bodies while modeling healthy eating behavior and attitudes. Increased physical activity reduces health risks and helps weight management. Nutrition education helps young children develop an awareness of good nutrition and healthy eating habits for a lifetime [27].
Psychologist Albert Bandura has defined self-efficacy as people’s beliefs in their capabilities to exercise control over their own functioning and over events that affect their lives. One’s sense of self-efficacy can provide the foundation for motivation, well-being, and personal accomplishment. People’s beliefs in their efficacy are developed by four main sources of influence, including (i) mastery experiences, (ii) vicarious experiences, (iii) social persuasion, and (iv) emotional states. High self-efficacy has been linked with numerous benefits to daily life, such as resilience to adversity and stress, healthy lifestyle habits, improved employees performance, and educational achievement [28].
The results showed that the mean scores of parents’ perceptions in children obesity of the pre-school children weight after the pre-experiment were higher than post-tested experiment. Parental self-efficacy beliefs embody an estimation of the degree to which parents perceive themselves as capable of performing the varied tasks associated with this highly demanding role. This result confirms that a studied of Ayfer Ekim [29] who reported that appreciation for cognitive factors associated with parental competence and satisfaction is increasingly evident in recent developmental research. In particular, parental self-efficacy beliefs have emerged as both a powerful direct predictor of specific positive parenting practices and a mediator of the effects of some of the most thoroughly researched correlates of parenting quality including maternal depression, child temperament, social support, and poverty. It means after the post-tested experiment, parents’ perceptions have evidence of the higher self-efficacy that their possibility of therapeutic intervention designed to alter competency perceptions among parents who are at-risk or who are currently experiencing difficulty in parenting is examined and avenues for future investigative work are suggested. Pre-school is an important period for the development of healthy lifestyle behaviors. Parents have a great influence upon a child developing healthy lifestyle behaviors [19].
Although obesity rates have leveled off in Thailand between 2003 and 2014, the rates of childhood and adult obesity remain high or approximately 17% and 36%, respective [30]. Parents of children who are overweight often fail to accurately identify their child’s weight status. This research has examined whether parental perceptions of child weight status are protective against weight gain during childhood using Albert Bandura’s Self-Efficacy Theory’ program was to examine whether parental perceptions of child weight and height statuses are associated. Albert Bandura’s Social Cognitive Theory emphasizes how cognitive, behavioral, personal, and environmental factors interact to determine motivation and behavior. According to Bandura, human functioning is the result of the interaction among all three of these factors [31], as embodied in his Triadic Reciprocal Determinism model.
While it may seem that one factor is the majority, or lead reason, there are numerous factors that play a role in human behavior. Furthermore, the influencing factors are not of equal strength, nor do they all occur concurrently [32]. According to the Social Cognitive Theory is composed of four processes of goal realization: self-observation, self-evaluation, self-reaction and self-efficacy. These components are interrelated, each having an effect on motivation and goal attainment [33]. Perceived self-efficacy mediates anxiety arousal that similar findings were also reported in later studies. The research results are consistent with the study results of Karineh.[34].
However, self-beliefs of efficacy is an important factor in human motivation [35]. This finding depended on the actual weight of the child; the association between perceiving one’s child as being overweight and future weight gain was similar among children whose parents accurately and inaccurately believed their child was overweight. Parental identification of child overweight is protective against further weight and height gain. Rather, it is associated with more weight and height childhood. Further research is needed to understand how parental perceptions of child weight may counter intuitively contribute to obesity.
Research on the single quasi-experimental method was to investigate the effects of a program for promoting and enhancing parents with of their perceptions to the expectations program for enhancing abilities and expectations toward self-efficacy in the pre-venting school children whose age ranged from 2 to 5 years old at the Child Development Demonstration Center, Faculty of Nursing, Khon Kaen University was administered with a sample size of 14 obese children at pre-school children and their parents at random were assigned. The sample group received the program comprising media, manual, video, and storytelling. Specify the research terms for each semester and data collected using the Child Weight Recording Form.
We analyzed statistically significant with the mean average, a t-test, and pre-test and post-test design was compared. It also provides support for the parent contributions’ abilities that they needed to take differences into consideration when planning and designing in their affecting programs for enhancing abilities to self-efficacy differently (p < 0.01). According to Bandura [36], there are five major sources. Which had a statistically significant difference at the level of .05, meanwhile this program could control child weight as targeted required number [37]. If the child has a taller stature or height than the average standard, it might show signage for nutritional disorders for 16 weeks on this food program research, differently [38].
According to the results of this research study are consistent with the study results of the Social Cognitive Theory proposes that individuals do not simply respond to environmental influences, but rather they actively seek and interpret information [39]. Individuals “function as contributors to their own motivation, behavior, and development within a network of reciprocally interacting influences”. Although Social Cognitive Theory covers many topics such as moral judgment and physiological arousal, research has been primarily focused on self-efficacy, or the beliefs regarding one’s capabilities of successfully completing tasks or goals, significantly [40].
Finally, this program promotes verbal or social persuasion and also affects parents with obesities’ perceptions of self-efficacy. It is a way of strengthening parents’ beliefs that they have what it takes to succeed. Their persuasion can provide a temporary boost in perceived ability. When it is effective in mobilizing a parent to action, and their actions lead to success, the enhanced self-efficacy may become more permanent. Children’s parents who persuade verbally that they possess the capabilities to master given activities are likely to mobilize greater effort and sustain it than if they harbour self-doubts and dwell on personal deficiencies when problems arise. This research shows that increasing the parents’ chance of success to provide with the research program for enhancing the protection of children with obesity. Unfortunately, it is more difficult to instill high beliefs of personal efficacy by social of children’s parents to persuasion alone than to undermine it unrealistic boosts in efficacy are quickly disconfirmed by disappointing results of children’s efforts.
Open access funding provided by Khon Kaen University, Khon Kaen Thailand. We gratefully acknowledge the financial support of the Department of Child Health Nursing Center, Khon Kaen University Fund Research Budget.
Information pamphlets for National Research Projects, Khon Kaen University, Department of Child Health Nursing, Faculty of Nursing, Khon Kaen University, and Kamalasai Hospital, Kamalasai District, Kalasin Province, Thailand for Health Research Ethics.
We are also grateful to the 14-children and their parents for assistance with their perceptions to moderate this paper and in that empirical data of the manuscript significantly.
We are also immensely grateful to Prof. Dr. Toansakul Tony Santiboon for his comments on an earlier version of the manuscript, although any errors are our own and should not tarnish the reputations of these esteemed professionals.
- World Health Organization (WHO). World Health Organization (WHO). Obesity. 2018 https://www.who.int/topics/obesity/en/
- World Health Organization (WHO). Obesity and overweight fact sheet N°311. WHO. 2015.
- Colquitt JL, Pickett K, Loveman E, Frampton GK. Surgery for weight loss in adults. The Cochrane Database of Systematic Reviews (Meta-analysis, Review. 8: CD003641.
- Dibaise JK, Foxx-Orenstein AE. Role of the gastroenterologist in managing obesity. Expert Review of Gastroenterology & Hepatology. 2013; 7: 439–451.
- Woodhouse R. Obesity in art: a brief overview. Front Hormone Res. 2008; 36: 271–286.
- Haslam DW, James WP. Obesity. Lancet. 2005; 366: 1197–209.
- Oxford: OUP Oxford. Obesity. Oxford handbook of medical sciences (2nd ed.). 2011: 180.
- Institute of Medicine. Early childhood obesity prevention policies. National Academies Press. 2011.
- World Health Organization (WHO). Obesity and overweight. 2020. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
- Center for Disease Control and Prevention. Childhood obesity causes & Consequences. https://www.cdc.gov/obesity/childhood/causes.html
- Department of Health, Ministry of Public Health. Obesity reveals threatening Thai children. 2018. https://www.thaihealth.or.th/Content/23671
- Nokdee C. Obesity reveals threatening Thai children. Thai Health Promotion Foundation. 2014. https://www.thai-health-promotion-foundation/1
- Rhee K. The role of parents in preventing childhood obesity. 2008. https://www.aapss.org/news/the-role-of-parents-in-preventing-childhood-obesity/
- Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review. 1977; 84: 191 – 215.
- Bandura A. Self-efficacy: The exercise of control. New York: Freeman. 1997.
- Bandura A. Social cognitive theory of personality. In L.A. Pervin& O. P. John (Eds.), Handbook of Personality: Theory and research. 2nd ed, 1998; 154-196.
- Hax G. Self efficacy and work related performance: A Metaanalysis. Psychological Bulletin. 2010; 124: 240-261.
- Bandura A, Barbaranelli C. Multifaceted impact of self-efficacy beliefs on academic functioning. Child Development. 1996; 67: 1206-1222.
- Bandura A. Moral disengagement: How people do harm and live with themselves. New York: Worth.
- Masten AS, Cicchetti D. Developmental cascades: Desired outcomes for children. Development and Psychopathology. 2010; 22: 491–495.
- Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932; 22: 55.
- Santiboon T. Appropriating characteristics of the 21st century teachers to transform of the Thailand 4.0 policies. African Journal of Pedagogy and Curriculum. 2017; 4: 48-64.
- Barlow SE, The Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2018; 120: S164-S192.
- Center of Disease Control and Prevention. Childhood Obesity Facts: Overweight & Obesity, Data & Statistics. 2019. https://www.cdc.gov/obesity/data/childhood.html
- World Health Organization (WHO). Noncommunicable diseases: Childhood overweight and obesity. 2020. https://www.who.int/news-room/q-a-detail/noncommunicable-diseases-childhood-overweight-and-obesity
- Mayo Clinic. Childhood obesity. 2020. https://www.mayoclinic.org/diseases-conditions/childhood-obesity/symptoms-causes/syc-20354827
- Department of Health. Preventing childhood obesity: Tips for parents. 2020. https://www.health.ny.gov/prevention/nutrition/resources/obparnts.htm
- Lopez-Garrido G. Self-efficacy theory. Simply Psychology. 2020. https://www.simplypsychology.org/self-efficacy.html
- Ekim A. The effect of parents' self-efficacy perception on healthy eating and physical activity behaviors of Turkish Preschool Children. Issues in Comprehensive Pediatric Nursing. 2015; 39: 1-13.
- Robinson, E, and Sutin, A. R. (2016). Parental perception of weight status and weight gain across childhood. Pediatrics. 137(5), May 2016, e20153957.
- Crothers LM, Hughes TL, Morine KA. Theory and cases in school-based consultation: A resource for school psychologists, school counselors, special educators, and other mental health professionals. New York: Routledge, Taylor & Francis Group. 2008.
- Wood RE, Bandura A. Social cognitive theory of organizational management. Acad Manag Rev. 1989; 14: 361-384.
- Redmond BF. Social cognitive theory components. 2010. https://wikispaces.psu.edu/display/PSYCH484/Social+Cognitive+Theory+Components
- Tahmassian K, Moghadam NJ. Relationship between self-efficacy and symptoms of anxiety, depression, worry and social avoidance in a normal sample of students. Iran J Psychiatry Behav Sci. 2011; 5: 91–98.
- Gecas V. Self-efficacy and social cognitive theories. 2004. https://wikispaces.psu.edu/display/PSYCH484/7.+Self-Efficacy+and+Social+Cognitive+Theories
- Bandura A. Self-efficacy. Encyclopedia of Human Behavior. 1994; 4: 71-81.
- Hong SA, Mongkolchati A, Chompikul J, Mo-Suwan L, Choprapawon C. Comparison of Prevalence of Nutritional Status of Thai Children in the First 2 Years of Life Using National and International Growth Charts. J Med Assoc Thai. 2016; 99: 58-64.
- Nestle: Good Food, Good Lift. The appropriate height for your kids. 2015. https://www.nestle.co.th/en/nhw/news/the-appropriate-height-for-your-kids
- Nevid JS. Psychology: Concepts and applications (3rd ed.). Boston: Houghton Mifflin Company. 2009.
- Locke EA, Latham GP. Building a practically useful theory of goal setting and task motivation: A 35-year odyssey. American Psychologist. 2002; 57: 705-717.